(General Hazardous Materials Behavior Model)
© 2001 by Ludwig Benner Jr .
Towson, Maryland USA, June 8, 2001
| The Story of GEBMO |
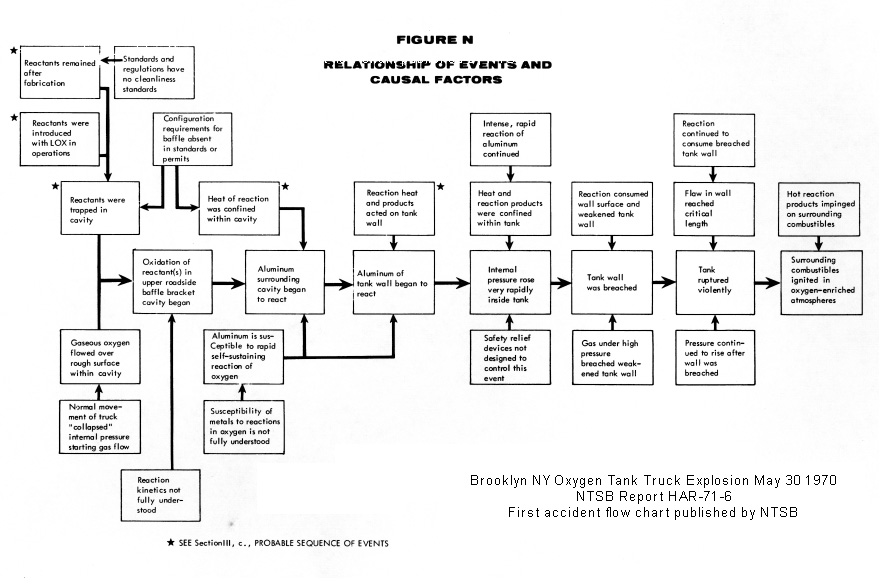
AbstractThis document presents my best recollections about the development of the D.E.C.I.D.E. and GEBMO models, now widely used in hazardous materials emergency response training and operations. In the absence of a diary, I have attempted to reconstruct the personal experiences that influenced the development of these models and the emergency response system built around them. Hopefully it illuminates the experiences that motivated me to find something better, and the inputs that influenced the development a better way. As you proceed, it will help to know that this work produced a new framework for thinking about hazardous materials emergencies, new response objectives, new incident decision processes, new ways for assessing response performance and above all, about a 90%+ reduction in casualties among emergency responders at hazmat emergencies. AcknowledgmentsI want to acknowledge the special contributions of Henry Wakeland, Director of the NTSB's Bureau of Surface Transportation Safety whose vision, leadership and encouragement played a major role in the accomplishments of the new safety levels for emergency responders in which I engaged for 10 years at the Board. Also thanks to John Reed, who as Chairman of the Board during the early years made the Board a very pleasant and rewarding professional experience for technical personnel, and to Member Louis Thayer who was especially helpful during my rookie year at the Board. Thanks to Tony Schmieg my first supervisor at the Board who give me special insights into highway traditions. Of course, very special thanks to Frank Brannigan of Montgomery College for the challenge and opportunity to access active firefighters' knowledge and ideas as they evolved, and to the students who patiently sat though some tedious sessions before I could make the new response concepts and their application clear to them. More thanks are due individual students at Montgomery College like Don Morrison and his mental movies insight, and to Mike Hildebrand who more than any other student grasped the significance of the new work and acted on it over the years. Also a special thank you to Charlie Wright for his unflagging encouragement during early days when these ideas were deemed too radical for the fire service, and for his subsequent extension of the ideas. Also a special thanks to Bill Meeker for his personal encouragement and support (and good times) at the Safety Board when the ideas were considered way out in left field by traditionalists. Also a special thanks to my staff at the NTSB, especially Tom Lasseign, Vic Hess, Becky Rote and Mike Hildebrand, whose views and inputs help refine the ideas that evolved. Special thanks also to Bob Graziano of the Bureau of Explosives whose efforts brought the new ideas before the emergency response community though AAR training programs, to Bill Black of the Federal Railroad Administration who was also open-minded about the regulatory implications of the work, John Zercher of CHEMTREC for his friendship and suggestions during the development process – especially the suggestion to give the process an acronym (which became D.E.C.I.D.E. and GEBMO), and to Martin Grimes and Tony O'Neil for their receptiveness to new ideas while in positions of influence at the NFPA. Lastly, thanks to my friend, Warren Isman, one of the risk bearing firefighters whose adept prodding of the risk creators helped so much to get needed changes implemented. Many others like Stan Hoffman of the Hazardous Materials Advisory Committee, Bill Hadden of the Insurance Institute for Highway Safety, Howard Fawcett of the NAS-Marine Board and Tom Hughes of the National Fire Administration who all helped spread the ideas To those who helped and are not mentioned my apologies – I should have kept a diary. IntroductionPersonal backgroundI am a chemical engineer. I also studied traffic management. I have worked within the domestic and international transportation industry much of my lifetime, primarily as a shipper or transporter of hazardous materials. My work from 1951 until 1970 involved the packaging, labeling, marking, documentation, transportation and regulatory compliance for hazardous materials shipments, ranging from small samples to shiploads. My responsibilities ranged from the preparation of specifications for hazmat containers to examining accidents to strive for continuous improvement in performance and efficiency. It also included service on industry advisory groups and committees, and the operation of rail and highway hazmat transports. That experience and a short period as a consultant gave me insights into the roles and responsibilities of all the parties involved in hazardous materials (hazmat) transportation by all modes My roles ranged from transportation engineer responsible for hazmat containers to General Distribution manager, responsible for the safety efficient and economical transportation of hazardous materials, and consultant to the carriers. In summary, I knew intimately all the players and all aspects of hazardous materials transportation until they became involved in accidents. Then they become someone else's responsibility to deal with and clean up. This was my experience and mindset during that era. The Conventional Wisdom in 1970The conventional wisdom of the time about the relationships among participants in the hazardous materials transportation process is important to understand to provide a context for the changes that followed. Both the transportation activities and the emergency response activities operated within the bounds of the prevailing conventional wisdom in their fields. The Federal regulatory agency also functioned according to the prevailing conventional wisdom about hazmat regulation that had evolved over a half century of safety efforts. Response responsibilityThe conventional wisdom in hazmat transportation was rooted in evolved transportation law. That law clearly delineated the responsibilities and accountability of entities engaged in transporting goods for hire. For example, terms of the bills of lading, which made the carriers responsible for the goods while in their possession, insulated shippers from any problems created by their shipments during transportation accidents. In other words, if there was a derailment followed by fires and explosions, that was somebody else's problem. The carriers, on the other hand, relied on equipment specifications to control hazmats in normal accidents, and on emergency response personnel to take care of any abnormal (accident) emergencies along their lines, with help from the Bureau for the Safe Transportation of Explosives (BofE), a nominally independent organization set up by the railroad industry to exercise safety functions for the carriers. And the responders accepted the responsibility for dealing with whatever might be thrown at them. One result was numerous fatalities and injuries among responders and bystanders, in hazmat accidents. TerminologyDuring this time, a shift in terminology was occurring. The term "dangerous goods" was the term of art for over 60 years, originating in railroad circles and tariffs for pricing transportation services. With the advent of the new Department of Transportation, a new term was coined – hazardous materials. The change shifted the focus from shipments to the materials in shipments. Largely unnoticed at the time, the changed focus resulted in subtle but important changes in the thinking about these shipments in transportation, as will be seen. Response objectivesTwo aspects of emergency responses should be noted. First as motor carrier traffic in dangerous goods increased, the emergency response responsibilities underwent a subtle change. Secondly, the conventional wisdom among emergency responders did not change. With the growth in truck traffic, the characteristics of hazmat emergencies began to change. They no longer occurred on private railroad property, but began happening on the doorsteps of local fire services, in less isolated settings. Thus the role of local fire and public safety services changed from one of guided participants in responses on private properties where the railroads were responsible for the outcomes, to emergencies in which they were solely responsible for the emergency response operations and their outcomes Meanwhile shipment sizes, including hazmat shipments, were getting larger and larger. Emergency responders were strongly influenced by the prevailing operational "attack and extinguish" philosophy of the fire services. The tactical objective was to "cool the tanks" with water above the liquid line to prevent what were becoming known as "BLEVES" or boiling liquid, expanding vapor explosions. The prevailing wisdom for developing guidance for hazmat responses was an "if-then" approach to the development of emergency response practices and their implementation. Diagnostics were not considered practicable, and besides, the BofE would be there to offer guidance if needed. Regulatory approachThe prevailing conventional wisdom influencing regulations was that safety could be achieved by basing rules on the inherent nature of the materials, and keeping them contained in their packaging in normal accidents. Properly describing, classifying, packaging, marking, labeling and documenting shipments occupied most of the regulatory energies. With the occurrence of the high-consequence accidents and casualties in the late '60s, the agency was beginning to become aware of regulatory shortcomings, and launched initiatives to provide emergency response advice, within the framework of the emergency response philosophy of the times.) NTSB ExperiencesIn May 1970 I joined the National Transportation Safety Board. At the time, the Board, under Chairman John Reed, former governor of Maine, was predominantly a technically oriented organization. With Mr. Wakeland's generous managerial and technical support, the Board became a major catalyst for change in the hazardous materials transportation field. The BoardThe Board started operations, within the U.S, Department of Transportation, under a 1966 act of Congress. Shortly after its formation, a number of hazardous materials railroad accidents involving hazardous materials produced significant civilian and emergency response casualties in all modes[1]. These accidents were investigated by railroad, marine, air and highway accident investigators, whose primary focus was on the operational aspects of the accidents. Railroaders focused on why the equipment derailed, for example. Highway investigators concentrated, for the most part, on the vehicles, roads and drivers. Under the leadership of Henry Wakeland, the Director of the newly created Bureau of Surface Transportation Safety, the Board investigators began examining more closely how the hazardous materials were escalating losses during the accidents. At Wakeland's urging, in mid-May of 1970 the Board hired its first hazardous materials specialist for his Intermodal group to give added emphasis to the losses attributable to the behavior of hazardous materials in such accidents. In 1973, during an overhaul of the Board's mandates, it became an independent agency of the Federal Government \ The Board's Intermodal GroupThe Intermodal Group consisted of a system safety specialist, a statistician, a psychologist and a chemical engineer (me). I functioned as the Board's Hazardous Materials specialist. Group members served as in-house consultants to Board modal investigators during investigation and to special study teams, and thus had the benefit of seeing cross-modal problems and issues in transportation safety. The serendipity among the Group members anticipated by Wakeland did in fact occur. One of the reasons I was hired was because of my interest in a risk-based approach to transportation safety, which Wakeland considered attractive at that stage in the Safety Board's surface transportation safety program. One of my first assignments was to develop a special study to examine risk concepts in dangerous goods transportation. That study, for which I was the principal author for the Board, with major contributions from Wakeland, was adopted in January of 1971.[2] It influenced changes ranging from statutory mission changes to emphasis on emergency responder safety emphasis by the Board. It should be read to gain insights into subsequent Board initiatives in the Hazmat safety field. At a Forum sponsored by the Transportation Association of America, the history of its evolution and elements of the study were discussed at length. As an introduction to issues like "testing hazardous materials regulations on the public" and the need for predictive analyses of risks, the Proceedings of the Forum is must reading, particularly Wakeland's introductory remarks. It was during that study that I first recognized the significance of the prediction problem confronting firemen during their on scene response efforts. The Board's prior hazmat experiencesThe Board had investigated accidents involving hazmats prior to my arrival, and had addressed the emergencies created by the hazmats in various ways. In December 1966, a self-powered passenger car collided with a fuel oil truck at a grade crossing, resulting in fire, death of 11 and injury of 28 passengers, and death of 2 train crew members. In this case, the Board made a recommendation to take lowest risk routes for hazard materials vehicles using grade crossings. Dunreith, IndianaA January 1, 1968 accident at Dunreith Indiana involved the explosion of an ethylene oxide car in a fire fed by flammable materials released during the wreck. At the time, the Bureau of Explosives -- an arm of the railroad industry -- was called on to direct responses to hazmat emergencies. The Board recommended study the problem of proper management of hazardous materials in train accidents, establishment of a national advisory data center for emergency responders, better markings on hazmat cars, reconsideration of the use of the Bureau of Explosives for hazmat safety rules, and a study of means to help local fire departments to upgrade their skills in handling emergencies created by hazmats in accidents. In that report, the focus was a lack of adequate knowledge and data to support local hazmat responses operations. The report coinciding with the motivation for a new mission of the new Department of Transportation, influenced the Department of Transportation and industry representatives to begin working on emergency information guidance manuals for responders, a new arena for regulators. Laurel MississippiA spectacular accident involving liquefied petroleum gas and what is now called the BLEVE phenomenon occurred at Laurel, Mississippi January 25, 1969 resulted in 2 fatalities and 33 injuries, destruction of 54 residences and 1350 damaged residences. The Board reiterated its recommendations in the Dunreith case, and proposed actions to keep tank car parts from rocketing into communities in accidents. This marked the beginning of a decade-long undertaking and studies to reduce the frequency of head punctures in tank cars used for transporting compressed, liquefied gasses. It eventually resulted, about 9 years later, in one of the most expensive transportation equipment retrofit programs in U. S. history, which reduced the incidence of these problems by over 95%, as predicted. Crete NebraskaA February 1969 accident at Crete Nebraska involving release of liquefied ammonia resulted in 6 fatalities and 35 injuries from exposure to the released ammonia. The Board recommended a study of ways to protect the public from exposure to hazmats released in accidents. Demands to do something about tank car failures did not develop quickly, but the need was being demonstrated with increasingly more compelling evidence. Glendora, MississippiA September 1969 accident involving vinyl chloride at Glendora Mississippi resulted in explosions and fire but no fatalities. The Board reiterated its Laurel recommendations to help local responders and reconsider reliance on the Bureau of Explosives to assure hazmat transportation safety. The Department of Transportation began a shift from private (BofE) to public safety control rules. By applying system safety principles to these accidents, Wakeland had provided the Board with a broad hazmat safety improvement agenda that recognized losses due to the hazmats involved and problems with emergency responses to those transport accidents Several specific changes were launched, retrospectively, but an overall "game plan" to achieve improved future hazmat safety performance had not you evolved. Such a game plan was the purpose of the Risk Concepts Study, STS 71-1 published in January 1971. The NTSB Risk Concepts StudyThe Board's study STS 71-1 titled "Risk Concepts in Dangerous Goods Transportation" reviewed the evolution of the US safety regulatory scheme, and enumerated the current difficulties they presented.[3] It then proposed a new framework for considering the full range of risks involved, their identification, evaluation and reduction, proposing further efforts to implement the concepts. Chaucey Starr's seminal 1969 paper[4]"An Overview of the Problems of Public Safety" was a significant influence on this report. The Study attributed the observed loss consequences to the underlying approaches to hazmat safety and regulatory approach, noted above, and the existing "system" rather than the performance of individuals involved in the losses. The focus on preventing hazmat releases left unabated the other loss-producing interactions in these accidents, leaving to chance the severity of consequences to populations at risk. The study delineated the difference between parties-at-risk (emergency responders, bystanders, transport system operators, other occupants of transportation pathways, nearby residents) and parties-in-interest - carriers, shippers, regulatory agencies, container manufacturers)! Thus it was the Safety Board that started the process of bringing the risk creators -- the shippers, packaging manufacturers, carriers and regulators -- face to face with the risk bearers whose lives and property were at stake when accidents occurred. Another significant innovation was the visibility and emphasis placed on the loss severity and exposure elements of risk. By highlighting these aspects of the safety paradigm, the Board added emphasis to the need to consider post-collision or post-derailment risk management and risk reduction. Another significant point made by the study was the need to analyze system risks. rather than focusing on the inherent properties of the materials. The immediate study aftermathThe Risk Concepts study came out after Crescent City, and was widely circulated, becoming an NTSB "best seller" according to NTIS. Reinforced by continuing serious hazmat accidents and their widespread publicity, its framework triggered serious reconsideration of the conventional wisdom and new interactions among all parties involved. They started talking and listening to each other. For example, at a Forum sponsored by the Transportation Association of America, the history of its evolution and elements of the study, its application and questions were discussed at length. As an introduction to safety policy issues like "testing hazardous materials regulations on the public" and the need for predictive analyses of hazardous materials risks, the Proceedings of the Exploratory Forum on Risk Concepts. is must reading, particularly Wakeland's introductory remarks. It was during that study that I first recognized the significance of the prediction problem confronting firemen during their on scene response efforts. The study influenced changes ranging from statutory mission changes to emphasis on emergency responder safety efforts by the Board. It should be read to gain insights into subsequent Board initiatives in the Hazmat safety field. The study also provided new criteria for investigating and analyzing what happened in accidents, from everyone's perspective. This occurred about the same time that the shippers and Federal hazmat transportation regulatory agency were developing the industry's responder assistance "hot line" that had evolved into the CHEMTREC operation at the Chemical Manufacturers Association. It should be noted that the information provided was based on the inherent properties of the materials. In my work at the Board, I began practicing what I was preaching. Using the Framework in the study, I began to expand the scope of my investigations to include events that occurred after a crash or derailment, including the processes employed by emergency responders. The first accident where this strategy was fully employed was a derailment in Houston Texas in 1971. Accidents influencing GEBMO developmentIn May of 1970, I began to observe personally the losses, which Mr. Wakeland had discussed with me, in accidents in which I conducted the investigation, supervised the investigation, or provided hazmat guidance to the investigators. Each played a role in the proposed changes in emergency response concepts, processes and guidance that evolved. Brooklyn New York.A May 1970 mysterious oxygen tank truck explosion in the yard of a Brooklyn New York hospital occurred two weeks after I joined the Board. I was assigned the investigation, and developed a flow chart of the accident process, showing its progression between the braking of the truck and the losses that occurred[5]. The Board adopted the proposed report with the flow chart. |
|
At the time, the conventional wisdom was that an accident was an unintended, undesired event which was probably ambiguous by design, since the term needed to cover so many different kinds of phenomena. Without realizing it at the time, I had depicted the accident as a process with various kinds of events. The effort to flow chart the Brooklyn accident precipitated some significant questions which bothered me as I became better acquainted with the NTSB investigation process. But that is covered in other papers.[6] It was significant in the development of the GEBMO model because it formed a process basis for my thinking about hazardous materials accident process models. Crescent City, Illinois.On June 21, 1970, I was assigned to the NTSB team investigating the Crescent City Illinois railroad accident. Included in the 15 derailed cars were nine tank cars loaded with liquefied petroleum gas. During the derailment one of the tank cars was punctured, and the leaking propane was immediately ignited, engulfing the other tank cars in the fire. A series of explosions of the remaining tank cars occurred, beginning about 1 hour following the derailment, resulting in the injury of 66 persons and the destruction of a number of buildings within the town of Crescent City. For three days, the town was immobilized. This occurred in a major media market and was a spectacular event for the media
The Crescent City LPG explosion, June 21, 1970.
|

|
The widespread distribution of the escaped materials and car pieces observed from the air also left an abiding impression on this investigator. It was clear that responders were powerless to change the outcome during the post derailment course of events in that accident. This accident raised questions about what could be done in emergencies involving these materials and quantities when they escaped from their "containers/" During the investigation I learned that firefighters were burned in explosions while pursuing their tactical objective - cool the tank shell above the liquid level to prevent a BLEVE[7]. It was a scenario that I was to see repeated often in subsequent accidents. In the Crescent City investigation, I did some quick approximations. As I recall, these tank car shipments contained around 2 billion BTUs of energy. When that energy was released, there was no way firefighters could put anywhere near the amount of water required to absorb that much heat energy on the ensuing fire. And because of the unpredictability of the tank ruptures at the time, it was impossible to tell when they would be faced with this massive heat output. This raised obvious questions about the tactical objective. It was unclear to me what responders to emergencies involving these materials and quantities could do when the contents escaped from their "containers" and what their response objectives should be. It was clear why the prevailing "attack and extinguish" approach could lead to disaster. The experience suggested to me that something was amiss with the guidance offered these brave firefighters. As we discussed this problem, John Zercher of CHEMTREC observed after the 1974 Oneonta NY derailment and LPG explosions, the best thing firefighters could do was to climb a hill and watch the explosions, because they would probably never see another one like this in their lifetime. Wow -- this was a " do nothing" option for the decision makers - totally foreign to the prevailing gung-ho mindset of the firefighting community at the time, and incidentally to the guidance offered at that time. In the Waco case, the question came up again. Waco GeorgiaSubsequent to the Study's release, I participated in 3 highway hazmat accident investigations including the Waco Georgia accident. Two firemen (attacking the burning truck wreckage), a wrecker truck driver and two civilians were killed by the exploding dynamite cargo in a semi-trailer van that had been struck by a car with subsequent fire. It demonstrated again problems with the warning system for providing responders data they needed to make their risk taking decisions. In this case both fire fighting and rescue concerns confronted responders arriving at the scene. The Board recommended, in September 1972, that NFPA develop new guidelines dealing with explosives in emergencies. and bring them to the attention of emergency services personnel at all levels. It called for special emphasis on assessing the situation on arrival at the scene, determining alternative courses of action, evaluating the risks associated with each alternative, and selecting the alternative which presents the minimum risks to people, facilities, and fire fighting crews and their equipment. With the responder casualties in this case, it was becoming clearer to me that there were common challenges for hazmat accident responders across modes. Another interesting point came emerged in that case: there did exist a precedent for advising responders to withdraw from fires if an explosive cargo was involved in the accident. Franklin County, MissouriIn December 1970, LPG released after a pipeline rupture in Franklin County Missouri ignited and produced an open air detonation. The explosion, equivalent to 100,000 pounds of TNT and fire resulted in extensive property damage within a 2 mile radius. This was the first reported case of this phenomenon. I raised questions in my mind about the regulatory classification scheme within which a hazardous material classed as a flammable could detonate like an explosive. It was not to be the last time a material not classed as an explosive material detonated. The implications for emergency responders, who depended on knowing the class of material they were dealing with, seem profound to me at the time. But a sample of one is not evidence enough to challenge the system. Berwick MaineAnother accident I investigated in April 1971 was the gassing of factory workers when a truckload of chemical was connected to the wrong receiving pipe at a tannery, and a fatal reaction occurred in the mixed chemicals. I had seen improper connections before, also with potentially lethal consequences, but the accidents were over before the responders could get involved. But it stuck in my mind - by then I was starting to think about describing the accident process observed in general terms so the lessons learned could be disseminated widely across industries. Gretna FloridaIn this August 1971 accident, a highway collision between a passenger car and truck resulted in hazmat containers in the truck shifting and being breached during the accident. Four people in the immediate vicinity of the accident were fatally gassed as the escaping methyl bromide/chloropicrin mixture contaminated the air around the wreck. As I consulted with the investigator about the hazmat behaviors, the dispersion of the gas in this and the Berwick cases, in the absence of fire, suggested to me that the range of harm from hazardous materials cargoes needed to be considered for all kinds of hazardous materials, not just for flammable materials and explosion threats. My inventory of dispersion issues was building rapidly. The Houston, Texas accidentA railroad accident in Houston on October 19, 1971 and subsequent public hearing provided another pivotal experience. A derailment and fire, followed by the explosion during firefighting operations of tank care containing vinyl chloride, killed one firefighter and injured 50 other individuals, mostly firefighters. Significantly, injury to a firefighter on a ladder pouring water on the fire, who was overwhelmed by the explosion, was captured on film and was given prominence in the media and throughout the emergency response and transportation communities. During the investigation process we learned that the emergency response personnel were doing what they were programmed to do by their training. No reasonable person could complain that the firefighters were stupid to do what they did. The casualties demonstrated -- again and very convincingly -- that their programming led to the casualties. The firefighter fatally injured by the hazmat explosion was the training officer. As I heard the on-scene officers describe what they did and why they did it they provided me with many new insights into specific needs for improving emergency responses programming if losses were to be reduced in the future. The response training did not provide decision making process guidance appropriate to the events during this post-derailment emergency. Clearly, something was amiss! The casualties to responders following existing guidance convinced me that it was the guidance that was untrustworthy, with potentially lethal consequences for those who acted in good faith on that advice. The report was issued in December 1972. The Board found that "The severity of the accident was increased by the abrupt rupture of the tank car and the lack of adequate training, information and documented procedures for identifying and assessing the threats to public safety." Threat assessment was introduced into the lexicon of emergency responders. I think it this accident and the information about the challenges faced by responders that brought to the forefront of my thinking the need to develop threat assessment concepts and procedures for emergency responders the if-then cookbook approach being pursued at that time by the DOT and CHEMTREC, focused on the properties of the materials, was not satisfying the need. This is discussed in greater detail in a 1990 paper[8]. Delta Air LinesA December 31, 1971 a pint of Molybdenum 99, a radioactive material with a 66.5 hour half life, escaped from its container in the cargo hold of a Delta Convair 880 enroute to Houston, TX. The aircraft carried 917 passengers before the spill was discovered and the aircraft was taken out of service. The incident was first detected two days later by a consignee who noted his shipment was contaminated while unpacking it. This incident raised a whole new set of transportation issues and eventually resulted in legislation governing radioactive materials shipments by air. East St. Louis IllinoisPropylene involved in this accident devastated a railroad yard and adjacent properties - including a school building in January 1972. Walking among the rubble 8 hours later impressed me with the energy that had to be released to do all the work (damages) I was seeing. The wreckage and damage pattern suggested that the propylene may have produced a low order explosion when it ignited, based on the nature of damages to equipment near the center of the explosion. After this accident, the Board recommended that cars carrying these commodities be treated as explosives cars in switching operation, and not be "humped" even though the cargoes were classified as flammable gases. The implications for response guide writers were interesting: treat these materials as explosives or gases? Lynchburg, VirginiaIn March 1972, a tank semitrailer truck overturned on a downhill curve on a mountainous road, and slid into a rock outcrop next to the highway, puncturing the tank. LPG released from the punctured tank killed three residents in a home in a valley below the wreck when the spreading vapor cloud ignited. As I viewed the topography at the scene, it became clear to me that these bystanders never had an informed chance to recognize or react to the threat from the LPG dispersion they faced. The experience raised more questions about warnings within the range of effects of some hazmat cargoes. New Jersey TurnpikeOn September 21, 1972, about 25 minutes after a highway crash and fire, a propylene tank semi-trailer tank exploded, with one piece rocketing 1300 feet in one direction and another piece 500 feet in the opposite direction. 28 persons were injured in the explosion while responders were on scene. The Board criticized the lack of understanding needed to predict the range of the hazard facing the responders, attributing the relatively few casualties in part to luck. Put up or shut upOne of the fire service experts with whom I explored my evolving insights and criticisms of the current emergency response guides for hazmats during these investigations was Frank Brannigan. An experienced firefighter and introspective thinker, he provided me valuable data about the fire service philosophies, perceptions and practices. He also was a valued source of information about radioactive materials and their behavior over the years. Brannigan's challengeBrannigan took vigorous exception to my radical thoughts about the inadequacy of the training approaches and materials, and especially my notion of challenging the conventional wisdom dominating the fire service's attack and extinguish mindset. In one moment of exasperation during one of our discussion he challenged me to prove myself. His challenge:
It was a fair challenge. With considerable trepidation, I finally agreed to teach a Fire Science hazardous materials course for him in his program at Montgomery College. That meant looking around at the material that existed to see what I might use, and developing a syllabus I would need to teach. Frank would provide the students to thoroughly challenge my ideas. The students provided not just an embedded conventional wisdom, but also illustrated for me what it might take to overcome that conventional wisdom with new ways of thinking. By then, I had some concrete ideas about what needed doing, so in the fall of 1973 I found myself standing before my first class of working firefighters attending a class at night to get required credits for their AA degree. .At the time, the most widely used texts for hazmat courses for firefighters were by fire service officers -particularly Bahme[9] and Meidl[10]. They reflected the conventional approach of describing the classes of materials, and some accidents to show what they could do. No general decision making process was described, nor was a structured threat assessment process defining data search, data interpretation, alternative outcome prediction, tradeoff consideration, and response action selection addressed, so I knew I would have to develop my own texts to cover the decision making process. So I did. Starting with Meidl's texts, I developed handouts to address the decision making process during emergencies, and to address the input data need to support that decision process. The handouts grew into a 70 page course book with 16 lesson outlines, called Hazardous Materials Emergencies, published for the 1976 class. The work was appended with a student work book with exercises to accompany each course session, and later still, an answer book was published showing school solutions to the exercises. But I get ahead of myself. 1973-1976 was a very busy period. Concurrent influencesAccident model developmentsConcurrently, when I started working for the Safety Board, I tried to learn how the "old hands" at the Board performed investigations. As I worked with different investigators in different modes, I was surprised -- and confounded -- by the different ways investigators viewed an accident, how they scoped their investigations, and how they actually did their investigations. Particularly vexing was the question of scoping the investigation. Hazmat accidents took varying times to come to a conclusion, and the sequence and timing of what happened during the course of the accident played an important role in the eventual outcome. Questions like what should be included in the investigation, and where did the accident start and stop were answered inconsistently. To try to come up with answers that could provide consistent guidance and results, I tried to document and formalize how investigators investigated accidents at the Board. As that effort progressed, I researched the available literature for a generalized model of the accident process that reflected what I was observing. Again, without recognizing the significance at the time, I tried to flow chart a generalized description of the accident process derived from my observations during cases in each mode, and from prior work in the literature. I found kinds of events that were common to all accidents, and that could be abstracted into a general accident model. That work resulted in an accident model I first documented and published in 1975[11]. Intervention pointsPart of the Board's mission was to make recommendations to prevent repetition of the accidents they investigated. This meant that there should be some strategy for identifying how to intervene in the accidents to change future outcomes. When I tried to add intervention points to the model that was evolving, I discovered that intervention ideas for the model were related to the intervention challenges during the emergency response decision processes. In order to know what intervention actions to take, one had to know the stage of the hazmat accident process at which intervention would begin. Aha! It also dawned on me that for emergency responders to intervene successfully, they had to know
If they could not change the outcome, as in Crescent City and elsewhere, why intervene? The D.E.C.I.D.E. and GEBMO modelsFrom mid 1972 to mid 1973, I got an investigation breather, as accidents tapered off. I started to pull all the ideas about the accident process, the intervention decision opportunities, the intervention decision making process and the outcome prediction needs together. In a March 1973 paper[12] I pointed out the emergency response problem, noting that risks to responders were 10 times as great to responders as to any others, and called for better understanding of the response process. As the accidents and classes continued, the process -- and problems -- became clearer to me. In late 1974 they had gelled to the point that I was able to produce a general decision model for hazmat emergencies. The original D.E.C.I.D.E. model looked like this: |
|
In the hazmat emergency response decision process, predictions are needed before decisions can be made about intervening in the unfolding accident process. From observations of how losses occurred during the accidents we investigated, the data needed for those predictions became visible. In hazmat emergencies we saw that these predictions depended on data about the hazmat and container present, container stressors, the potential behavior of the stressed container and its contents, the potential behavior of the contents if released, where they will go if released, exposures they will impinge if they get where they are likely to go, what harm they will do to the impinged exposures.-- both people and objects. The, decision makers had to identify what options they had to change the outcome during that process. For each option, the same predicative effort was needed to determine if the changed outcome justifies intervention. These elements were incorporated into a General Behavior Model of hazmats in transportation accidents. The model was designed to help guide the threat prediction process, so it should be viewed as a threat prediction model for use during hazmat emergencies. John Zercher suggested that it would be nice to have an acronym to help people remember what it was. I chose acronym GEBMO -- an acronym that met with considerable derision when first sprang on my students. Who would possibly give serious consideration to -- GEBMO? That work formed the general basis for the course and supporting handouts in 1976, in a textbook [14]) used at Montgomery College. They included the first version of the GEBMO model. The rough and tumble of the Montgomery College courses in 1973 - 1975 helped me refine and expand the ideas derived from my observations of what happened in hazmat accidents where responders suffered casualties. I was in the unique position of testing my hypothetical models against observed events during subsequent accidents with investigators, with John Zercher at CHEMTREC -- who was dealing one-on-one with responders during accidents -- and with the very cooperative students in the course. The students particularly provided additional insights, such as the idea suggested student Don Morrison of forming a "mental movie" to help the on-scene commander visualize what was expected to happen at the site, from any point in time forward. This became an essential concept for applying the predictive threat assessment process model. I t helped show on-scene commanders how they needed to develop their "scripts" for their mental movies. In other words, it was needed to shift responders away from the "chem-card" if-then cookbook advice mode toward a "think your way through this new situation" mode. As I focused on the hazmat emergency response decision process, my observations indicated that the management process at a hazmat emergency was not that much different from management of other risky processes in which I had participated or had managed. I tried to capture a generalized description of that process, in a flow chart format, for several reasons.
|
The 1976 GEBMO version published in Hazardous Materials Emergencies was streamlined; each element was described in increased detail in the book:
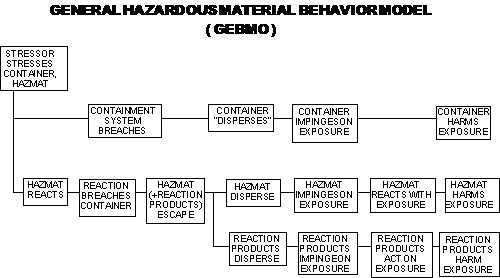
Accidents like Wenatchee and prompted the introduction of the "hazmat reaction products disperse" branches in the more recent GEBMO model.) I suspect more changes will be forthcoming if someone is willing to step forward to assume responsibility for keeping the model updated after I retire. Third a flow chart could provide a working tool so everyone was talking the same language during individual emergencies. I don't know how often this has occurred. Finally, it provided guidance for safety professionals to broaden the range of safety approaches they might use to produce better future outcomes. As more accidents were investigated with this approach, new opportunities for improving predictive tools arose. I had been trying to formalize ny work by documenting the ideas about making decisions in Hazardous Materials Emergencies as the work progressed. The ideas were passed out as handouts to students as they evolved. In 1975 Martin Grimes and Tony O'Neil decided to publish the finished paper in NFPA's Fire Journal[13] to give the information widespread exposure in the fire service community. It was republished in NFPA's Publication SPP-49, Hazardous Materials Transportation Accidents, in 1978. That paper is posted on the internet at http://www.bjr05.net/papershm/DECIDE.htm It describes each element of the decision making process, and the rationale supporting each step. In it, the emergency process model with possible intervention points was published in flow chart format for the first time. During this period, NFPA staff was actively engaged in the problems, and produced several publications describing what was happening. One of the most important was the NFPA Technical Information Bulletin 1-74, which was a progress report on NFPA's study of hazardous materials accidents. Acknowledging that the report might be considered alarmist by some, Mr. Grimes explained that the report was issued so that "at least, fire fighters should know the realistic risks they might have to face." It is my personal opinion that his action was an unusual display of courage, in that some of the major supporters of his organization were producers and shippers of the commodities that were creating these problems. Continuing accident feedbackAs the ideas for hazardous material emergency response guidance to support the decision making needs of responders were evolving I had the unique opportunity to test and refine my ideas against what was observed in subsequent accident investigations. I was fortunate to be an "outsider" doing this because I was not bound in any way by the experiences and implicit assumptions built into the responders' perceptions, viewpoints and expectations. Each accident and many class sessions added something new or forced me to refine the ideas about the D.E.C.I.D.E. and GEBMO models and others that evolved, over the period I taught at Montgomery College. until 1977. Benson ArizonaIn May 1973, sparks from railroad brake shoes ignited the wood floor of a box car, which resulted in the explosion of military bombs in that and a number of adjacent box cars over a five mile stretch of track. Fortunately the explosions occurred in a deserted area. minimizing damage. The incident demonstrated the difficulties responders would face in trying to control the fire - inside a closed box car - before the bombs exploded. Interestingly, not very many bombs detonated, raising questions about the lingering risks posed by the ones that had been heated but had not exploded. A whole new element had to be considered for the decision process. Hmmm. Kingman, ArizonaOn July 5, 1973, a tank car containing LPG parked on an industrial rail siding in near Kingman, started leaking during unloading. The leaking gas ignited, knocking two unloaders off the car. The fire began to intensify, engulfing the loading rack and the top of the car. The fire department began trying to get water on the car to cool the tank, when about a half hour later the tank car exploded, The fireball extended 15- to 200 feet from the car, leaving 13 dead and 95 injured. While the Board did not investigate this accident, since the car was no longer in transportation, we followed the investigation closely. . Pan Am Boston 707 FreighterThis accident occurred over a 20 minute span in November 1973, as nitric acid started a fire in the cargo area after the aircraft was airborne. As our investigation proceeded, I observed that the emergency response challenges for the crew were not unlike challenges in other hazmat accidents with respect to the decision making process involved. The crew was confronted with something they had never experienced, and had no basis for recognizing that hazmat were involved -- they first thought they were dealing with electrical overheating of fire, and acted on that assumption until other symptoms appeared. The commonality included the hazmat detection, threat prediction and assessment, selection of action options and the influence they had on the evolving outcome. The closed environment was different, but the accident fit the models that were evolving in my mind. The lessons learned were learned again a generation later in the ValuJet crash into the everglades. 1974 was a bad year. Oneonta, New YorkAnother "Crescent City" type accident occurred in a rural setting in February 1974. Still the LPG explosions and fire injured 54 firemen and members of the press during the emergency response. It was their first experience with this kind of emergency. The firemen had not been trained to cope with an emergency of this magnitude. This is the accident to which Zercher referred when he observed that firefighters should climb the nearest hill to watch it, because they would never see another one like this again, and there wasn't anything they could do about it. The accident produced some spectacular photos, widely published and circulated in the fire service. The fire service community leadership was gradually but surely beginning to lose patience with these kinds of accidents and casualties, and the risk creators. Decatur IllinoisIn July 1974, a switching accident in a railroad yard released isobutane from a tank car, It vaporized for about 10 minutes, exploded at 5:03 a.m. and damaged 700 homes, making some uninhabitable. A nearby school was one of the most severely damaged buildings, and 31 commercial establishments reported damages. Losses were estimated to be $18 million. 7 railroad employees near the explosion were killed, and numerous injuries were reported outside the railroad yard. This was one of those accidents about which responders could have done nothing to change the course of events. Had they had arrived on scene and pursued their customary tactics, more casualties would have occurred. . Wenatchee WashingtonThe following month, on August 6, 1974, a contents of a 10,000 gallon tank car detonated unexpectedly in a switch yard. The monomethylamine nitrate in solution was classified as a flammable solid. Here was another example of a classification scheme failure, based on the detonation. It acted like a duck, but it wasn't classified as a duck. The implication for everyone handling the shipments were readily apparent. Standing in the deep crater of a flammable solid detonation left a strong and lingering impression on this investigator. What if firefighters had responded to a wisp of smoke visible during the few minutes before explosive reaction and approached it in the customary manner? The complication of the responders' threat prediction challenge due to the hazmat classification reinforced my perception of the need to change the basis for response guidance then being circulated. . Mustang OklahomaOn September 1, 1974, colliding trains resulted in the release of isobutane from a punctured tank car, with ensuing fire. Firemen evacuated eight families in a 1 mile area, but allowed the wreckage to burn. A first. They will probably never see another fire like that one. Houston TexasOn September 21, 1974, another explosion in a railroad switch yard when a tank car carrying butadiene was punctured during railroad yard switching operations. The butadiene vaporized, ignited and in 2 to 3 minutes, exploded. One person died, and 235 were injured in the blast. This one blew before responders could get on scene. The Board reiterated its recommendation that these tank cars be treated like explosives in railroad switch yards. The observed range of effects in these accidents was really bothering me more and more as I pondered the implications for emergency responders. Eagle Pass TexasIn April 1975, a tank semi-trailer with LPG separated from the truck tractor, struck a concrete abutment and ruptured, releasing the LPG which vaporized, ignited and exploded, fatally injuring 16 and burning 51 others in the area. The Board recommended research to try to reduce the severity of such accident. Emergency response was not addressed in this case. In 1975, the Board created a new Hazardous Materials Division, of which I was designated Chief. After that I did not do many more field investigations. Glen Ellen IllinoisIn May 1976 ammonia escaped from a tank car derailed in a populated suburban Chicago community, and I did get on scene there. 14 persons were treated for exposure to the released ammonia. I noted with great interest that in this accident, persons who remained indoors were well protected against injury from exposure to the released ammonia, providing evidence that evacuation was not always the only option to be considered in hazmat accidents. In the report, the Board stated that when hazardous materials are present, firemen might have to abandon their traditional "attack ad extinguish" approach and adopt alternative emergency response procedures. I felt comfortable proposing that to the Board because I know by then from my work and consultations that options were available. Houston TexasIn September 1976, a tank-semitrailer load of anhydrous ammonia was released in a single truck accident on an interstate highway cloverleaf bridge, resulting in 6 fatal exposures, hospitalization of 48 and treatment of 100 others. The ammonia dissipated fairly rapidly. It was not a good year for ammonia transportation. The emergency response was not investigated because there was not much that could be done to combat the widespread dispersion of the vapor cloud around the clover leaf intersection before it naturally dissipated that day. Belt MontanaDerailing cars in this November 1976 railroad accident crashed into fuel storage tanks adjacent to the track, starting fires that burned for 12 hours. Several explosions occurred as the fire burned the derailed cars and nearby buildings. Firefighters were unable to determine the contents of the cars involved for more than 8 hours after the crash. Because it happened in a remote area, the accident did not receive much publicity. However, it did prompt serious dialogue among responder, carrier and shipper experts about the communication of needed data about the shipments involved in these accidents. Rockingham, North CarolinaThis March 1977 derailment involved challenges for the emergency response involving a radioactive material shipment. It resulted in a Board special study of released in 1979 calling on a critical review of all existing emergency response plans to determine their adequacy. In this accident, the fear factor aroused by the presence of a radioactive material container seem to create unnecessary stresses, in my view. It emphasized the need for better predictive threat assessment capabilities. Pensacola, FloridaA November 1977 derailment accident resulted in another release of a tank car load of anhydrous ammonia, 2 fatalities, 46 injuries and the evacuation of about 1000 persons. The Board noted that the preplan helped responders act effectively when they intervened, and again reported the lack of information on how to determine the potential danger zone of exposure to released hazardous materials. Another occasion when the wide geographic range of the gaseous threat posed special challenges to the responders. Youngstown, FloridaThe February 1978 derailment near Youngstown Florida was the first involving the release of liquefied chlorine in large quantities. The released gas killed 8 and injured 138 others. A three mile long gas cloud formed after the release. The cloud gave no discernible indication of its lethality to exposed victims. We kept seeing these accidents where there was little responders could do, due the large areas affected and the speed with which they were affected. It added pressure to take action to prevent the releases in the first place, or alt the very least, reduce the release rate from breached containers of these liquefied gaseous commodities. Waverly TennesseeThis February 1978 derailment and explosion turned out to be the turning point among emergency response disasters. It was the last one in which firefighter fatalities occurred during the response operations. 16 died and 43 were injured on the second day after the accident, when a tank car was being handled during reconsiders' efforts to reduce the residual risks posed by the damaged car full of LPG. It was also the case from which I developed the Time/Loss analysis technique for assessing the performance of emergency responders.[16] The Waverly case was the case used to illustrate the method. Crestview, Florida14 persons were injured by hazmats released during this April 8, 1979 derailment. The derailment occurred adjacent to a waterway, creating grave environmental problems during the cleanup operations. The report dealt extensively with emergency response issues, ranging from on-scene commander identification, dissemination of guidelines, evaluation of response preparedness and others. The M.A.P.S. ProjectObservations of threat assessment problems during these accidents suggested that the mapping of past spills might be helpful to responders trying to figure out where released hazmats might migrate. The Board developed and then began publishing its Spill Maps series.[17] The intent was to use them for other purposes too, such as validating spill model predictions that were evolving at the time, and for data about the range of effects for various risk assessment projects like routing guidance, etc. It may not be entirely clear to the casual observer, but much of the effort by the Board's Hazardous Materials Division was to encourage implementation of the D.E.C.I.D.E and GEBMO models. Implementation of the modelsThe course developed at Montgomery College formed the basis for the instruction of over 150,000 firefighters by the railroad industry in years that followed. For several years after 1979, when the instruction became widespread through efforts of the Association of American Railroads, Federal Emergency Management Association and others, to my knowledge no emergency responders trained in the elements of the D.E.C.I.D.E. process were fatally injured or disabled by hazmats in transport accidents. Rather than bearing risks 10,000 tunes greater per hour of exposure than others, the risk levels for responders declined to background levels for this activity. The ultimate result was what is now known and apparently widely taught as the D.E.C.I.D.E. process for hazmat and other emergencies where intervention can make a difference in the outcome. The D.E.C.I.D.E. process was applied experimentally to pilot emergency training in later years, with some apparent success. The D.E.C.I.D.E. and GEBMO models were used to identify needed changes in a state's emergency response agencies' assigned roles in accidents. I would be interested in other applications. The publications containing these materials were copyrighted, solely to try to control distortion of the concepts by well intended but inadequately researched and tested proponents. Royalty-free licenses were and will always be granted to anyone who wanted to use the material to improve the lot of any emergency response personnel without personal profit. I was paid well at the Safety Board while the material was being developed, and the improved performance has been very rewarding. They are now posted on an internet web site with a library of my publications. More details about other's efforts will be addressed in a future paper. [2] View study at http://www.bjr05.net/papershm/sts71abs.html [3] View study at http://www.bjr05.net/papershm/sts71.html [4] See Chauncy Starr's seminal work on societal risk in An Overview of the Problems of Public Safety, presented to the Symposium on Public Safety - a Growing Factor in Modern Design at the National Academy of Engineering, May 2, 1969 [5] See flow chart at http://www.bjr05.net/models/loxchart.jpg [6] See MES 75, et al at http://www.iprr.org/Papers/MES75.html [7] See LP GAS EXPLOSION, Kingman AZ July 7 1973, published by NFPA. 12 firefighters were fatally injured in this one. [8] See SAFETY TRAINING'S ACHILLES HEEL found at http://www.bjr05.net/papers/AchillesHeel.htm [9] see Fire Officer 's Guide to Dangerous Chemicals, ,Bahme, Charles W., N.F.P.A., Boston,MA,1972 [10]See Flammable Hazardous Materials, Meidl,J.H.,Glencoe Press, Beverly Hills,CA 1970 and his accompanying volume Explosive and Toxic Hazardous Materials [11] See 1975 paper Accident Investigation: Multilinear Events Sequencing at http://www.bjr05.net/papersa/MES75.htm [12] See HAZARDOUS MATERIALS TRANSPORTATION: CURRENT AND FUTURE ISSUES posted at http://www.bjr05.net/papershm/hmtissues.htm [13] NFPA Fire Journal, volume 6:9, July 1975. See article posted at .http://www.bjr05.net/papershm/DECIDE.pdf [14] HAZARDOUS MATERIALS EMERGENCIES, first published by Lufred Industries in 1976. It is posted for viewing as a PDF file at http://www.starlinesw.com/product/HME76.pdf [15] HAZMAT INVESTIGATIONS, is one of four investigation booklets originally published by Fire Protection Publications. It is now available from the Emergency Film Group as part of a video set, see the bottom of the page for separate pricing), or bulk orders are available from the author, [16] The Time /Loss Analysis method for assessing emergency response performance is described in a publication found at http://www.starlinesw.com/product/Guides/MESGuide07.html [17] The NTSB Spill Map program is described in a paper posted at http://www.bjr05.net/papershm/MAPS.html |
{kind=link}