|
When
one considers that there are at least .5 differing accident perceptions, 44
reasons for an accident investigation, at least 7 different investigation
processes, at least 6 basic and 22 supporting methodologies, and at least 3
types of work products, one gets insights into the range of choices available
to investigators. Add to these choices the undefined scope of investigations
and the resultant additional variations in resultant decisions by
investigators, and the impossibility of achieving reproducible investigative
results becomes unmistakably clear.
Sometimes
more than one set of choices was observed in the investigations of a single
accident. For example, following one accident, nine separate investigations
were conducted. An obvious question arises: why didn’t one investigation
with one investigative output serve everyone’s need for an
explanation
of the accident? The linking of several investigations of one accident was not
addressed in any accident manuals reviewed. Witnesses have been observed to be
questioned as often as five times: what
is the likelihood of getting identical statements each time? Did all the
investigators have . access to all the residues or debris that survived the
accident, even after destructive testing had occurred? In multiple
investigations, who did what testing? These kinds of questions suggest a need
to consider the larger question: why not one investigation? The answer seems to
lie in the differences in perceptions of the accident phenomenon and resultant
perceptions of “safety,” which drive different persons to seek
different information from the accident to serve their narrow purposes.
Another
relationship concerns applications of investigative findings for evaluation
purposes. Not one of fourteen major accident investigation manuals treats the
relationship between investigations and “safety” predictions.
Validation of “safety” performance assumptions on which
countermeasures are instituted is still apparently considered the domain of
“researchers.” While this linkup has been examined in the highway
and hazardous materials safety fields, (15,16,37) actual use of the predictive
analyses and logic by investigators during the planning and initial stages of
an accident investigation was observed only in two actual cases.
APPLICATION
OF FINDINGS
The
findings have spawned development of a new potentially unifying framework for
accident investigations and safety, with an accompanying new methodology for
investigators. The framework and use of the methodology has been taught with
games that simulate the investigative procedure. The principles and methodology
have been applied to achieve improvements in hazardous materials emergency
response decision making.
THE
NEW FRAMEWORK
The tentative new framework can be described most clearly by referring to an
orchestra and a musical score for a symphony. (38) It is based on the process
perception of the accident phenomenon, because that perception most nearly
seems to reflect realities observed in accident investigations .
An
orchestra consists of many musicians and instruments which must work together
to produce a melodious output. When these “actors” play a symphony,
they work from a plan (the score) that specifies what each musician and each
instrument must do during the entire symphony. If all adhere to the plan,
within close tolerances, the music envisioned by the composer will be
reproduced successfully, and the purpose of the activity will be achieved. But
if something occurs to disturb the musicians and keep them from achieving their
intended performance, some sour notes, or possibly even disruption of the
symphony can occur. For example, a perturbation like the collapse of the
conductor could stop the music. The disturbance can be viewed as being similar
to an “accident.”
Sometimes,
there is no score or plan, as when musicians get together for a “jam
session.” During such sessions, the musicians improvise the music they
play. If they are skilled and experienced, their music will be melodious and
pleasing most of
the
time. They may have to stop occasionally when they lose the beat, or misplay
notes. If unskilled musicians try to engage in “jam sessions,” the
results are more erratic, and the sessions will be disrupted frequently because
of coordination and timing problems, as well as sour notes. These interruptions
are unintended, but they occur. They too can be viewed as
“accidents.”
Conceptually,
these analogies parallel activities in which accidents occur. Activities are
conducted in a way that achieves a dynamic equilibrium (melodious music) among
the interacting actors (musicians) engaged in the activity (performance.) This
dynamic equilibrium, or homeostasis(17) among the actors requires constant
adjustive(18) interactions within certain tolerances(19) to proceed in the
temporal and sequential order demanded by the activity to achieve a successful
outcome. . While the activity is in the homeostatic (or “at risk”)
state, the actors interact within the required time and spatial boundaries,
undergoing continuing changes of state. These changes of state occur in
response to actions designed into the activity, or in response to changing
relationships among the actors, as when a sour note occurs. When an actor does
not adjust to a perturbation and the new state needed to sustain homeostasis,
and the activity is disrupted with some harm, the music stops. The
transformation from the homeostatic or the “at risk” state to the
unintended harmed state is analogous to the “accident process.” The
beginning of the “accident” process is the perturbation to which an
actor had to adapt within the required time and spatial constraints, but did
not. The end of the accident can be viewed as the newly harmed state of the
involved actors. Harmed state is that state in which an actor can no longer
continue the function required by the activity to sustain homeostasis, or which
requires ameliorative treatment .
The
analogy provides insights into relationships between safety and accident
investigation. The role of managers or “activity designers” is to
devise the “score” that actors (animate and inanimate) engaged in
the activity can follow to achieve the desired outcome, and to staff the
activity with skilled actors that can follow the “score.” Safety
analysts’ predictive role is to identify passages in the score that are
likely to give the actors problems, and either get the score changed, provide
better instruments, or give the musicians plenty of practice so they can play
the passages successfully. Accident investigators monitor the activity’s
performance; they need to find out what the score was, and explain the accident
(transformation) process which occurred in terms of the homeostatic state, the
perturbation(s) that occurred, the adaptive reactions, the successive changes
of state that ended in the harmed state(s) and the time or spatial constraints
on the actors. Another logical safety function would seem to be the monitoring
of continuing performance to determine how well the safety controls are
working, and whether other difficult passages are indicated by some sour notes
that did not end in accidents., i.e., ”near misses." In any performance
of the score, there is a nonzero probability that the musicians will have an
“accident.”
However, these accident scenarios must be understood before their probabilities
can be estimated or reduced with adequate certainty. This means that the
accident “scores” should be available to the activity
“composers” and analysts if the safety efforts are to be adequate.
It also means that “accident scores”-—the investigative
outputs—- should relate to the composers and the analysts scores.
A
NEW METHODOLOGY
Techniques used by the composer of the symphony can be adapted to accident
investigation. A composer predictively specifies the timing, duration and
nature of the actions for each actor in the orchestra, so that when they
interact, their efforts will produce the desired musical sounds. The format
used for these specifications is a graphic display of concurrent actions by
each actor in the orchestra, using symbols arrayed in what might be described
as a multilinear events sequences flow chart. This format provides for all the
ingredients needed to display an accident process flow chart--including the
actors, their actions relative to a time reference and relative to other
actors’ actions, and a sequential order for displaying these actions. By
tracking the actions (changes of state) of each actor involved in an accident,
and establishing time relationships among these actions, investigators
reconstruct the accident process. A “score” for the accident
process can be developed by recording these retrospectively derived actions on
a comparable multi-linear events sequences flow chart.
This
concept has led to an investigative methodology based on principles related to
the above discussion. The principles and methodology help to discipline
accident investigations by providing generally applicable criteria for
investigators to self-evaluate their investigative tasks and outputs during an
investigation. The most significant principles follow. (20)
Think
events:
an event is one action by an actor, linked to a change of state. This principle
forces the investigator to structure accident data into events “building
blocks” used in graphic displays of the accident sequences; focuses the
data search on actors involved in the accident; and concentrates attention on
what each actor did from the beginning of the accident to its end.
Think
event sequences
>:
this principle forces an investigator to fit the events derived from the data
into their temporal and spatial order. The sequential tracking of actions by
witnesses is another application of the principle, because it helps the
investigator structure the interview in a way that assures access to all the
witness’ observations or concerns.
Make
mental movies:
this principle provides a framework for arranging the events sequences of
several actors into a visual referent in which the continuity of sequences can
be tested by the investigator. Gaps in the movie indicate unknowns that the
investigator needs to resolve to fully understand or explain the accident. The
technique also screens out data that do not fit into the movie, and thus
minimizes the non-sequiturs that might be reported. Movies provide for the
practical implementation of an important investigative Law:
“Everyone
and everything always have to be someplace doing something.”
The
Law demands that a complete investigation account for each actor involved in
the accident, even if the actor was passive or “just resting;”
however it does not require that every actor be reported. The controlling
criterion is the “change of state” for events recorded on events
flow charts.
Advancing
time:
This principle requires investigators to establish the times for each event
recorded, and is the basis for the time logic testing used to qualify entries
on events flow charts. Every entry on a chart must be tested for the validity
of its placement relative to other events. This is done by establishing the
relative timing of events pairs known to the investigator, based on where and
when an actor did something during the accident or on physical laws that govern
sequential behavior. The positioning of an event on the events flow chart is
disciplined by an advancing time scale, so proceed/follow relationships among
events pairs are not violated. The time test and positioning of each event
acquired during the investigation, as it is acquired, constitutes a real-time
quality control test for ordering either observed or inferred events discovered
by the investigators. The constant application of this principle as data is
acquired is of special value in that data validity is quickly tested, and early
delineation of gaps in the understanding of the accident process remains
visible until the gaps are resolved. This further focuses the data search
efforts, facilitates data organization, and guides the recording of data during
the investigation. With an arrow convention to show the flow of events with
time, a crucial defect in other investigative processes is overcome.
These
principles have been organized into an investigative system that is based on
graphic representations of the accident phenomenon. The system incorporates a
TIME
LINE
to
discipline the positioning of events sequences in these displays; an
EVENTS
MATRIX
for
the orderly array of each actor’s actions; an
ARROW
CONVENTION
to
show the flow of valid proceed/follow interactions among the actors; and a
COUNTERMEASURE
TAB
technique
to identify candidate countermeasures that would change the accident
“score.” The system is illustrated in Appendix G. (22)
INVESTIGATION
PROCESS SIMULATIONS
The investigative process has been incorporated into four accident
investigation games that simulate the accident investigation process. (22)
These games replicate the development of an accident investigation plan in a
team investigation process; the acquisition of a witness’ complete story
during an interview; the development of a debris testing plan; and the
organization, testing and reporting of accident data during a report evaluation
exercise. These simulations have enabled students to identify and articulate
criteria to guide investigators during accident investigations, and to develop
a common basis for evaluation of investigative programs and deliverables.
Another
result of the simulations has been the clarification of specific deficiencies
in present investigative methods, which will probably have the long term effect
of bringing about changes to overcome
these deficiencies in the students’ organizations.
IMPROVING
EMERGENCY RESPONSES
The principles and methods described have been applied to identify safety
problems with emergency responses to hazardous material accidents, and to
improve performance of the firefighters involved in those emergencies. In a
1971 hazardous materials accident investigation (21) firefighters’
actions and decisions were tracked to find out what happened, using some of the
events display methods that were in early stages of development. The tracking
disclosed flaws in the decision making process that were linked to the way the
f ire-fighters had been programmed to deal with such emergencies. After
discovering these flaws, ways to overcome them were developed by predictively
tracking, step by step, the actions of hazardous materials cargoes, hazardous
materials containers, firefighters’ actions and decisions, and their
interactions with potential victims. When these actions were displayed
graphically, gaps in the emergency response process became visible. An orderly
process model was “composed” for the emergency, for the hazardous
materials behavior in emergencies, and for the resultant decision making
process required of firefighters. (20) The D.E.C.I.D.E. decision model is
gaining increased’ acceptance, and is becoming a basis for teaching
hazardous materials emergency decision making to firefighters. (39) The payout
for the effort has been a substantive change in attitudes and tactics in the
firefighting community, and an apparent decline in the casualty rate where
these methods have been applied.
The
models have provided another benefit for investigators. They have helped
investigators organize their investigative tasks in team investigations and
have helped focus the data search during investigations on data related to the
model. This has been accomplished without sacrificing the discovery potential
gained from the use of the events charting-based methodology.
These
results occurred, in large measure, because the author explicitly identified
his perception of the accident phenomenon on which he based his investigations
and work products. This experience suggests that articulation of one’s
perceptions of the accident phenomenon will provide useful criteria for self
evaluation by accident investigators. This experience also suggests that if
these perceptions of the accident phenomenon are not made explicit, attempts to
reconcile the widely divergent views about safety and accident investigations
hold little promise.
CONCLUSIONS
It
is clear to the author from this research and its applications that there is an
urgent need for unifying perceptions of the accident phenomenon and for
disciplined accident investigation methodologies that will overcome practical
and theoretical uncertainties facing accident investigators. Unless present
diverse perceptions are made visible, attempts to gain acceptance of the need
for reconciliation of diverse views are not likely to be supported.
To get these debilitating differences resolved, certain actions seem to be
needed.
1. Individuals
practicing safety activities should reexamine their perceptions of the accident
phenomenon, and then explicitly report that perception in the work products
that it influences. This would include investigative reports, program
evaluations, safety analyses reports, and similar work products. This action
would have the initial effect of forcing articulation and disclosure of these
perceptions. It should have a collateral effect of driving divergent
perceptions toward a ‘consensus as the effectiveness of work products
based on different perceptions become visible. In addition, it would have the
immediate effect of providing disciplining criteria for the work products
produced .
2. Accident
investigators must reexamine their investigative methodologies, and then
explicitly specify both the accident perception and the methodology used in
each reported investigation to produce the deliverables offered. This action
would have the effect of making visible implicit criteria for
investigator’s decisions about accident scope, data sought, analysis
methods and information reported. This should also have the longer term effect
of demonstrating the benefits of each methodology, based on the utility of the
outputs produced with each methodology. In addition, the perceptions and
methods, if reported, would put users on notice about the known difficulties
with each, identified in this research.
3. Persons
performing secondary investigations, using primary data reported by accident
investigators from field observations, should report both the accident
perceptions on which their work is predicated, and also the perceptions on
which the primary data was predicated. This would reduce the potential for
misuse of primary investigative data in secondary investigations. It would also
help secondary investigators self-evaluate their work products.
4. Research
should be initiated to develop a “best” accident investigation
methodology based on unifying safety, accident and methodological perceptions
and concepts. The methodology should not be an adaptation of methodologies from
other disciplines, but rather should be derived from the unifying safety,
accident and related concepts. This research would transcend any single public
or private agency’s interests, so it is not clear who should sponsor such
research. The “best” methodology should serve the greatest number
of users, whose perceptions of their needs may be reshaped if the first three
actions are implemented.
5. Accident
investigation program managers should reexamine their personal perceptions of
the accident phenomenon, and then explicitly specify the perceptions on which
their programs are predicated. This should have the effect of providing
criteria for operating and assessing all the elements of an investigative
program, as well as rationalizing the outputs. It could affect the nature of
accidents investigated, as well as the methods specified for the programs. This
action would probably provide a strong incentive to strive toward unifying
perceptions of the phenomenon in
Figure. 1 that does this. These actions can all be taken by individuals, except
for number 4. This means there is no valid reason for not getting started.
The
views expressed are those of the author and do not necessarily represent the
views of the National Transportation Safety Board.
REFERENCES
<1. US
National Transportation Safety Board, “Risk Concepts in Dangerous Goods
Transportation Regulations” Report NTSB STS 71-1, 1971
2. Haddon,
W. Jr., Suchman, E.A. and Klein, D., “Accident Research”, Harper
and Rowe, New York 1964 (Section 1)
3. Readers’
Forum: “Why do accidents happen?” Job Safety and Health, Aug. 1977
4. National
Highway Safety Advisory Committee “Highway Safety Data.” A report
to the Secretary of Transportation, June 19, 1979
5. Benner,
L., “Crash Theories and Their Implications for Research.” American
Association for Automotive Medicine Quarterly Journal, Jan. 1979
6. Jacobs,
H.H., “Conceptual and Methodological Problems in Accident
Research.” in Behavioral Approaches to Accident Research, Association for
the Aid of Crippled Children, New York, 1961
7. Fontenot,
B.P., personal communication.
8. Benner,
L. “D.E.C.I.D.E. in Hazardous Materials Emergencies.” Fire Journal,
69:4, July 1975
9. US
National Transportation Safety Board, “Inquiry Manual-Aircraft Accidents
and Incidents.” NTSB Order 6200.1, Washington, DC 1975
10. Johnson,
W.G., “Accident/Incident Investigation Manual.” ERDA7620. US
Government Printing Office, Washington, DC 1976
11. American
National Standards Institute, US Standard Method of Recording Basic Facts
Relating to the Nature and Occurrence of Work Injuries, ANSI 216.2—1962 (Rev.
1969) New York 1962
12. “Feasibility
of.securing research—defining accident statistics” Safety Sciences,
Dept. of Health Education and Welfare, National Institute of Safety and Health
Publication No. 78180, Sept. 1978
13. Haddon,
W. Jr., “Reducing the Damage of Motor Vehicle Use.” Technology
Review 77:8, Aug. 1975
14.
McGrew, D.R., “Traffic Accident Investigation and Physical
Evidence.” Thomas, Springfield, IL 1975
15 Hall,
W.K. and O’Day, J., “Causal Chain Approaches to the Evaluation of
Highway Safety Countermeasures.” J. Saf. Res. 3:1 1971
16. US
National Transportation Safety Board, Letter to Secretary of Transportation
transmitting Safety Recommendations 1769 through 17611, October 20, 1976
17. Pask,
G., “Interaction between Individuals: Its Stability and Style.”
Mathematical Biosciences 11, 1971
18.
McGlade, F.S., “Adjustive Behavior and Safe Performance.” in Ferry,
T.S. and Weaver, D.A., “Directions in Safety”, Thomas, Springfield,
IL 1976
19. Blumenthal,
M., “Problem Definition: The Driving Task in the System Context.”
Behavioral Research in Highway Safety, 2:1, Spring 1971
20. Benner,
L., “Hazardous Materials Emergencies” Lufred Industries, Inc.,
Oakton, VA 1976
21. US
National Transportation Safety Board, “Derailment of Missouri Pacific
Railroad Company Train 94 at Houston, Texas, October 19, 1971”
NTSB RAR—72—6, 1972
22. Benner,
L., “Four Accident Investigation Games Simulations of the Accident
Investigation Process.” Lufred Industries, Inc. Oakton, VA 1979 .
23.
Ames, J.S., “Aircraft Accidents: Method of Analysis.” Proceedings
of National Safety Council, 17th Safety Congress, 1928
24.
Heinrich, H.W., “Industrial Accident Prevention McGraw Hill, New York 1936
25. Thorndyke,
R.L., “The Human Factor in Accident US Air Force School of Aviation
Medicine, Project Report, Project No. 21—30—001, 1951
26. US
Dept. of Health, Education and Welfare, Public Health Service, “Uniform
Definitions of Home Accidents.” Washington, DC 1958
27. “Fault
Tree Analysis as an aid to Improved Performance” AMC Safety Digest, US
Army Materiel Command, May 1971
28. “Fault
Tree for Safety” D57133, The Boeing Company, Seattle, WA 1966
29. Suchman,
E.A., “A Conceptual Analysis of the Accident Phenomenon” in
Behavioral Approaches to Accident Research, Association for the Aid
of
Crippled
Children, New York 1961
30. Baker,
J.S., “Traffic Accident Investigator’s Manual for Police”
Northwestern University, Evanston, IL 1963 (Revised 1971)
31. Haddon,
W. Jr., “The changing Approach to the Epidemiology, Prevention and
Amelioration of Trauma: The Transition to Approaches Etiologically rather than
Descriptively Based.” American Journal of Public Health 58:8, Aug. 1968
32.
Surry, J. “Industrial Accident Research” University of Toronto,
Toronto, Ontario, Canada, 1969
33. Johnson,
W.G., “The Management Oversight and Risk Tree” prepared for the US
Atomic Energy Commission under Contract AT (043)821, Feb.1973 34. Benner,
L. “Safety Risk and Regulation” Proceedings, Transportation
Research Forum, Vol. XIII, No. 1, Chicago, IL 1972
35. Wigglesworth,
E.C., “A Teaching Model of Injury Causation and a Guide for Selecting
Countermeasures” Occupational Psychology 48:2, 1972
36. Leplat,
J., “Origin of Accidents and Risk Factors” paper presented on a
Seminar sponsored by the Swedish Work Environment Fund, Stockholm, 1975
37 Joksch, H.C. Reidy, J.C. Jr., and Ball, J.T., “Construction of a Comprehensive
Causal Network, Phase III, Final Report, Vol. I” Center for the
Environment and Man, Inc. Windsor, CT 1977
38
Benner, L., “Risk Responsibility and Research” paper presented to the
Symposium sponsored by the American Chemical Society Council Committee on
Chemical Safety, Chicago, IL, August 26, 1975.
39 Wright, C., “Railroad and Emergency Response Personnel: A Cooperative
Effort” presented to Hazardous Materials Workshop, 106th Annual
Conference, International Association of Fire Chiefs, Kansas City, Mo.
September 17, 1979
40. US
National Transportation Safety Board, “Improving Survivability in
Hazardous Material Accidents” Report HZM 795
41. Dieterly,
D.L., “Accident Analysis: Application of the Decision/Problem State
Analysis Methodology” AFHRL Technology Office, NASAAMES Research Center,
Moffett Field, Ca. 1978 (In publication)
42. Manual
of Aircraft Accident Investigation, Fourth Edition, International Civil
Aviation Organization Document 6920AN/855/4, Montreal, Canada 1970
REASONS
FOR INVESTIGATING ACCIDENTS
AS
REPORTED BY ACCIDENT INVESTIGATORS
|
determine cause
prevent accidents
prevent
similar accidents
required
by safety department
generate
statistics
determine
fault
find
violations .
establish
liability
settle
workmen’s compensation claims
verify
hypothesis
grind
an axe
satisfy
public curiosity
evaluate
a regulation
satisfy
a boss
satisfy
the employees
find
out who is to blame
find
out what went wrong
have
to fill in report
determine
subrogation chances
settle
insurance claim
assess
losses
train
students
|
> determine
causes
determine
probable causes
find
causal factors
identify
recommendations
improve
system
upgrade
operations
develop
training materials
improve
training
assign
damages
to
do cost/benefit analysis
understand
phenomenon
support
legislation
confirm
predictions
restore
confidence in system
fulfill
research contract
support
civil litigation
bring
about changes
restore
reputation
defend
civil suit
prosecute
violation
earn
a living
sell
ideas
|
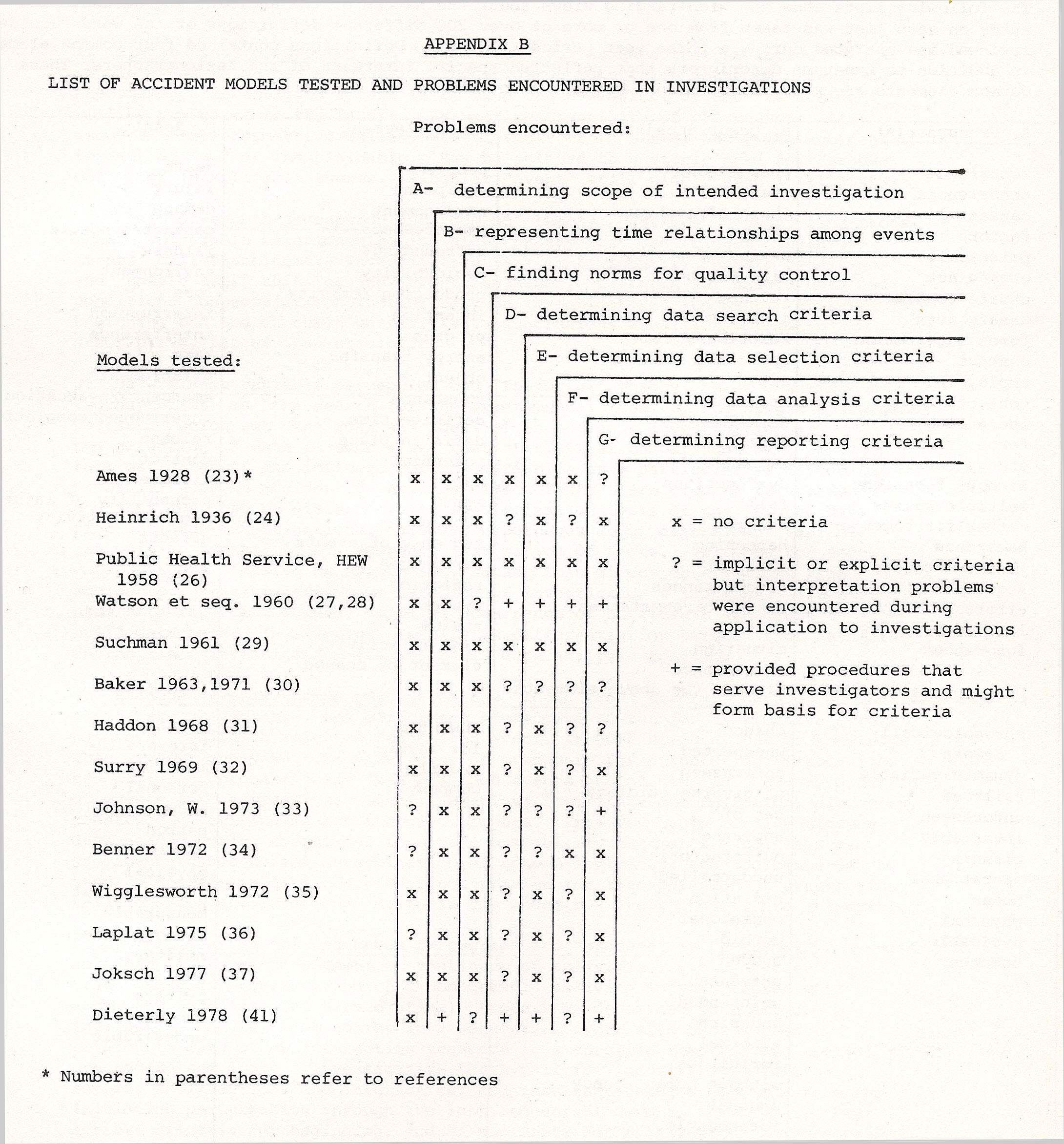
LIST
OF ACCIDENT MODELS TESTED AND PROBLEMS ENCOUNTERED IN INVESTIGATIONS
Problems
encountered:
APPENDIX C
ELEMENTS
OF ACCIDENT DEFINITIONS
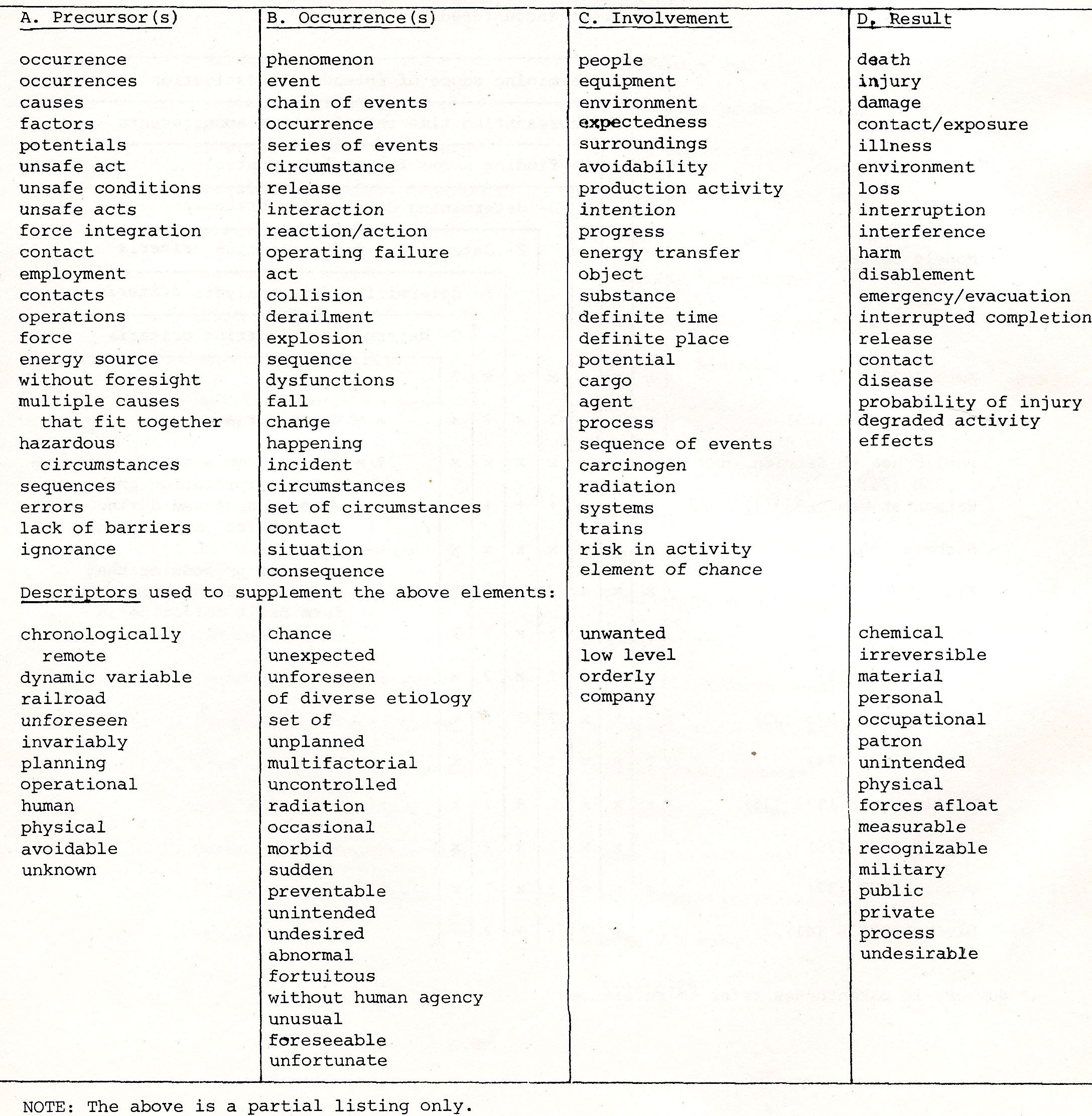
The
following lists show the wide ranging views about the nature of the accident
phenomenon. Each entry on each list was taken from one or more of over 200
different definitions of the word “accident” reviewed and analyzed
during a three year period (19758.) Definitions containe8 four common elements
in addition to numerous descriptors that reflected special interests of the
lexicographers. These common elements are precursors, occurrence(s),
involvement, and result
SUMMARY
OF ACCIDENT PERCEPTIONS AND THEORIES
1. Single
event perception and “cause”_theory
. Assumes that an accident is a single event which has a “cause.”
Investigator identifies cause to understand phenomenon. Investigative task is
to find cause, correct it and the accident will be prevented in the future.
Assumes replicability of phenomenon. Also assumes someone/something failed, was
at fault or to blame; otherwise accident is “act of God” or
unexplainable. May be related to historic need for “scapegoat” for
inexplicable events. Singular “event” still widely used in
literature.
2. .Chain-of-events perception and “domino” theory.
Assumes “unsafe” conditions create vulnerable relationships in
which “unsafe act” can trigger “chain—of-events”
called accident. Investigative task is to identify “unsafe
conditions” and “unsafe acts” that “caused”
events sequence. Criteria for unsafe acts and conditions unspecific;
conclusions rely on investigators’ judgment. Criteria for beginning and
end of chain unspecified. Conclusions usually symptomatic and descriptive,
rather than etiologic.
3. Determinant variable perception and “factorial” theory
Best described by Thorndyke (25) as “the search for the experimental
ideal of the single independent variable” which set “the goal and
ideal of an accident investigation as the gathering of data in such a way that
statistical comparisons will permit fair estimates of the influence of the
variables in a particular factor on the probability of an accident.”
Assumes common factors are present in accidents and that they can be discerned
with statistical analysis of the “right” data from accident
investigations. Assumes hypotheses about determinant variables can only be
identified by secondary examination of facts. Criteria for scope, data, outputs
dictated by hypothesis, rather than direct observations from accidents.
Requires extensive exercise of investigator’s judgments; often uses data
reporting forms. Requires occurrence of sufficient accidents to build data
base. In practice, results in differentiation between fact gathering during
field investigation and secondary data analysis function.
4.
Branched events chains perception and “logictree” theory.
Assumes accidental events are predictable, and structures predictive
search for alternative events pathways leading to selected “undesired
event, through speculations by knowledgeable systems analysts. Follows rules of
procedure for structuring speculations and assigning probabilities in a
branched events chains display. Demands ordering of events into accident
sequences. Displays facilitate communication, discovery, constructive
criticisms and technical inputs. Provides basis for identifying data needed
.during operations to update probability estimates. Displays can provide
guidance during investigation of actual accidents, and accidents can be used to
upgrade predictions. Does not provide for incorporation of events time
relationships and durations; criteria for undesired event choices are
unspecified.
5. Multilinear events sequences perception and “process” or ”p-theory.
”
Assumes accident is transient segment of continuum of activities; views
accident as a transformation process by which a homeostatic activity is
interrupted with accompanying unintended harmed state. Process is described
with actions by interacting actors, each acting in a sequential order with each
sequence related to each other interacting sequence in a specific temporal and
spatial proceed/follow logic. Investigative tasks call for identification of
the actors, their actions and interactions and resultant changes of state from
the initiating perturbation through the last sequential harm to the actors.
Prescribes criteria for beginning, end of accident; for data search; select4on;
recording; organization and testing. Display provides “time
coordinate” to discipline events timing relationships, and hypothesis
generation method, in addition to benefits of “logic tree” displays
described above.
APPENDIX
E
SUMMARY
DESCRIPTIONS OF SEVEN ACCIDENT INVESTIGATION PROCESSES
1. 0ne—person
process
.
One investigator performs all investigative functions, from data gathering,
interpretation and analysis, to reporting of findings. Also answers questions
arising during investigation. Tasks usually governed by reporting forms or
check lists which investigators must interpret and satisfy. May involve coding
of entries. Outputs usually brief verbal or narrative reports, or completed
accident report forms. Recommendations usually not made, or if made, are
shallow. Investigative procedures usually insubstantial.
2.
Intraorganizatinal
ad hoc team
process.
When accident happens, investigative team is formed within organization,
staffed by regular employees without substantive investigative training.
Usually teams search for chain of events, unsafe acts or conditions.
Investigative duties often subordinated to other duties after initial cursory
inquiries. Outputs usually internal reports of “cause(s)” with
shallow recommendations because of self interests of team members. Team
disbands after investigation is completed. Investigative procedures usually
meager.
3.
Intraorganizational standing team process
.
Predesignated team performs full range of investigative tasks, often involving
testing or examinations. Team usually includes one or more extensively trained
investigators with investigative experiences. Outputs usually are narrative
reports of “cause(s)” with reasoned, objective recommendations for
improvements in non-management areas of the organization’s activities.
Team members often able to implement improvements before report is issued.
Investigative procedures usually provided.
4.Multiorganizational
ad hoc team
Participants designated after accident occurs;
disbanded after investigation is completed. Used by both public and private
sector organizations. Investigators usually detailed to team for duration of
investigative effort. procedures governing tasks range from sketchy to
comprehensive. Draws on mixed talents of investigators to achieve adequate
investigation. Investigators usually trained. Outputs usually are narrative
reports of “causes” with mixed quality recommendations that depend
largely on project manager and team members, rather than procedures.
5. .
Multi-organizational standing team process
One organization organizes team formation, using representatives from several
other organizations or groups to investigate a series of accidents. Typified by
multi—disciplinary investigation teams from several cooperating
universities under contract to government, or teams from several companies
investigating a kind of accident plaguing an industry. Investigators often
trained on thejob; often assisted by experienced investigators on teams. Teams
usually focus on specific kinds of accidents to understand them better.
Methodologies usually reflect academic disciplines of investigators. Outputs
are narrative reports, usually comprehensive, often supplemented with
substantial tabulated or other data. Team dismissed at end of project.
6. .
Judicial investigation process
Special task force assembled and operated under the direction of a
distinguished jurist, often of national prominence. May be directed by jurist
in jurisdiction within which accident occurred. Investigation relies primarily
on witnesses’ testimony; may involve some technical testing or analyses.
Process governed by judicial procedures, rules of evidence and adversary
methods. Usually associated with an accident of national concern. Outputs are
usually narrative reports of “cause(s)” with recommendations, but
may also include criminal or other legal proceedings against parties at fault.
7.Legislative Investigation process
Investigation initiated by legislative entity acting in legislative or
oversight capacity. Usually involves investigation by legislative staff,
consultants. Investigation relies principally on witnesses’ testimony
before legislative subcommittee, and hearing records. Outputs are hearing
records, narrative committee report, and sometimes new legislation. procedures
of legislative body govern investigation.
APPENDIX F
EXAMINATION
TECHNIQUES USED IN ACCIDENT INVESTIGATION
1. Visual
inspection for residues, deviations from norms, deformations, etc.
2. Chemical
analysis methods, including chromatographic, infrared, wet chemical analyses,
pH tests, miscibility tests.
3. Thermal
analysis methods, including “temperature bars” differential thermal
analyses, decomposition or polymerization temperature analyses.
4. Radiographic
methods, including x—ray, gamma ray scans, carbon dating, emission
measurements .
5. Structural
analysis methods, including engineering calculations of force distribution or
changes; rotational analyses.
6. Force
vector analyses, based on Newton’s law of equal and opposite forces and
directions of deformation.
7. Dimensional
analyses, including comparative analyses of new vs. present dimensions .
8. Energy
traces, including energy flow, stressor/stressee analyses, thermodynamic
analyses.
9. Electrical
analyses, including circuit, conductivity, static charge, sneak circuit analyses.
10. Metallurgical
testing, including grain microphotographs, yield mode patterns, strength and
hardness tests, bend tests, ductility tests.
11. Crystallographic
analyses, including xray diffraction, formation conditions, types of crystals
present.
12. Reconstruction
of surviving parts, as with mockups, sequential break—up analyses .
13. Char
analyses, such as determination of char depth, char patterns, and char
composition versus known standard specimens and exposures.
14. Fault
tree analysis, for speculation on how the condition observed might have come
about.
15. Pressure
analyses, including vapor equilibrium, reaction pressure and velocity,
rate-of-pressure-rise-and—effects experiments .
16. Scenario
modeling techniques, such as events charting.
17. Flash
point tests for flammable liquids, dusts, powders.
18. Incubation
tests for etiologic and infectious agents, carcinogen, etc.
19. Buoyancy
tests for density determinations, mixing rate estimates.
20. Flow
tests, for viscosity, angle of repose, air entrainment effects.
21. Toxicity
tests, such as LD
50
and
LC
50
animal
tests, skin corrosivity tests, asphyxiation concentrations, blood tests.
22. Corrosion
tests, such as inches per year (ipy) rates, stress corrosion cracking tests.
INVESTIGATIVE
SYSTEM BASED ON GRAPHIC REPRESENTATION OF ACCIDENT PHENOMENON*
4
key Investigation System Elements
1. The TIME LINE to discipline the sequencing of events: to ______________________________________________________
2. The
EVENTS
MATRIX
to display events and their chronological relationships:
| one
actor + one action = an EVENT |
to ______________________________________________________
Actions ----->
Actor A
Actor
B
Actor
C
etc.
3. The ARROW CONVENTION to show the interactions among actors and to test the logic of the display:

4. The COUNTERMEASURE TABS to identify risk-reducing action options:

* Copyright © 1979 by LUFRED INDUSTRIES, INC. All rights reserved. Reproduced with permission.
|
 - - - - - -Last updated on Wed, Aug 8, 2012
- - - - - -Last updated on Wed, Aug 8, 2012